

ivermectin


I thought that we had all decided that ‘SARS cov2’ presented no risk of death or severe disease in the unvaccinated, under 70’s, yet we healthy freedom fighters still seem to be totally obsessed with ivermectin, early interventions and prophylaxis for a ‘disease’ that presents very little threat to us. (Many of us would say this is no virus and no covid nor any threat at all).
I had never heard of IVM before and now suddenly not a bad word can be said about it, it is apparently the cure for everything, it’s totally safe (have we heard that before?) and everyone is popping it like sweets or trying to sell me some. I thought I’d have a little look into it.
Ivermectin, ‘Wonder drug’ from Japan: the human use perspective by Andy Crump and Nobel laureate Satoshi Omura.
My comments in italics; The players; Merck, the WHO, the UN and the World Bank
The origins of ivermectin as a human drug are inextricably linked with Onchocerciasis (or River Blindness), a chronic human filarial disease caused by infection with Onchocerca volvulus worms. The parasites are transmitted via the bite of infected blackflies of the genus Simulium, which breed in highly-oxygenated, fast-flowing rivers and watercourses. In the human body, immature larval forms of the parasite create nodules in subcutaneous tissue, where they mature into adult worms. After mating, female worms can release up to 1000 microfilariae a day for some 10–14 years. These move through the body, and when they die they cause a variety of conditions, including skin rashes, lesions, intense itching, oedema and skin depigmentation.
In the early-1970s, the disease was endemic in 34 countries: 27 in Africa; 6 in the Americas; and 1 in the Arabian Peninsula. The World Health Organization (WHO) later estimated that 17.7 million people were infected worldwide, of whom some 270,000 were blind, and another 500,000 severely visually disabled (according to wiki there are now 15 million people infected and 800,000 with some vision loss). Does this disease affect only those who live near rivers? Is susceptibly to morbidity caused by a bite influenced by overall health and nutrition? Would it be more helpful to focus on these points?
How do we know the worms are causing the morbidities and blindness and are not merely associated with them? Could there be a possible health benefit to people in having them, just like the proliferation of bacteria is beneficial in eating dead cells? Are the morbidities themselves caused malnutrition, toxins or vaccines?
By 1973, Onchocerciasis had been recognised by the then head of the World Bank, Robert McNamara, as a major disease of massive health and socioeconomic importance and one in dire need of combating in West Africa, and he became the key agent for change.
Spraying was initially used against this parasitic disease It was a very ‘vertical’ programme, mainly coordinated through the World Bank and other UN agencies, with multimillion dollar contracts given to a US-based helicopter company and to an American chemical company for the insecticides. Species have evolved over millennia to be part of interconnected and interdependent ecosystems. Blanket spraying of a particular species with insecticides will not only upset this balance but also cause toxins to build up in the food chain and affect the microbiome and nutritional quality.
Originating from a single Japanese soil sample and the outcome of the innovative, international collaborative research partnership to find new antiparasitics, the extremely safe and more effective avermectin derivative, ivermectin, was initially introduced as a commercial product for Animal Health in 1981.
The initial trials on Ivermectin These trials were independently organized and funded by Merck, with a staff member, Dr Mohamed Aziz, previously of WHO, being the caring and committed driving force behind them. Dr Aziz started the study in Senegal;
Initial clinical studies in 32 Senegalese subjects have demonstrated the efficacy of ivermectin in Onchocerca volvulus infection (river blindness). Although O. volvulus microfilariae (an early stage of worm development) in skin snips were not reduced in number after single oral doses of 5 micrograms or 10 micrograms/kg body-weight, they were greatly reduced in all subjects after single oral doses of 30 micrograms or 50 micrograms/kg and were eliminated completely in 6 of th 8 subjects who received the 50 micrograms/kg dose. All subjects tolerated the drug well. Transient pruritus which did not require treatment was observed on the day the dose was given in 2 of the 8 subjects after the 30 micrograms/kg dose and in 4 of the 8 who received the 50 micrograms/kg dose. Ivermectin produced no abnormal laboratory results. Efficacy and tolerance of ivermectin in human onchocerciasis (The study shows IVM decreased presence of worms but not that IVM had overall benefits nor improved survival outcomes. The cause of vulnerability to worms was not addressed. The presence of worms could have been beneficial)
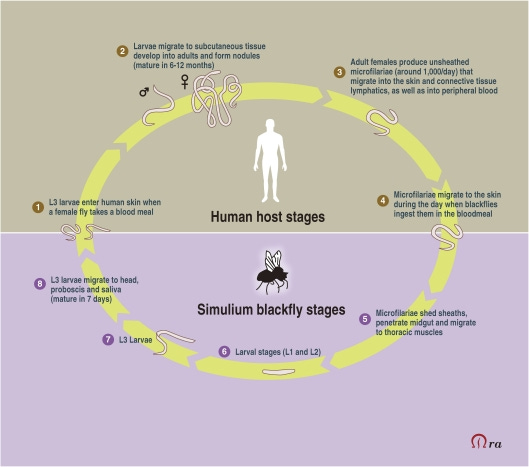
(The ‘leopard skin’ appearance of the microfilariae migrating to the legs varies during times of the day according to when the black flies are mostly likely to bite and enter the blood stream for the next stage of the cycle.)

For a long time, it was believed that ivermectin was contra-indicated in children under the age of five or who weighed less than 5 kg, as there was a fear of neurotoxicity, the drug possibly being able to cross the as yet not fully developed blood/brain barrier. However, evidence has emerged that is probably not the case.
In the human body, ivermectin exerts a peculiar and singular effect that remains poorly understood… The prevailing school of thought is that ivermectin actually interferes with the ability of microfilariae to evade the human immune system, resulting in the host’s own immune response being able to overcome the immature worms and so kill them.
In reality, the renewed interest in fighting tropical diseases, including the involvement of the pharmaceutical industry, which has become increasingly evident over the past three decades, and which has saved lives and improved the welfare of billions of people, notably the poor and disadvantaged in the topics, can be traced back to the 1987 introduction of ivermectin for use in humans. According to a recent report, International Federation of Pharmaceutical Manufacturers & Associations (IFPMA) data show that the global pharmaceutical industry provided over $9.2 billion in health interventions (medicines and equipment) between 2000–2007 alone, benefitting 1.75 billion people worldwide. The hitherto unprecedented donation of ivermectin in 1987 can rightly be seen to be the origin of this philanthropic outpouring.

Since the inception of the Mectizan Donation Programme, Merck has donated well over 2.5 billion Mectizan® tablets for Onchocerciasis treatment, with in excess of 700 million treatments authorised. Currently, some 80–90 million people are taking the drug annually through MDA in Africa, Latin America and Yemen. A further 300 million total treatments have been approved for lymphatic filariasis, with around 90 million treatments being administered annually. At present 33 countries are receiving ivermectin for Onchocerciasis and 15 for Lymphatic filariasis.
Consequently, around US$4 billion worth of ivermectin tablets have been donated to date (surely there must be a payback?*). In 2010, Ecuador became the second country in the Americas to halt River Blindness transmission. It is hoped that transmission of the disease in the Western hemisphere will be stopped by 2012—a goal that will have been achieved thanks to twice-yearly MDA with ivermectin. Lymphatic filariasis is targeted for global elimination by 2020, and, if all goes well, Onchocerciasis may well be eliminated from Africa soon thereafter. This indicates that development of an effective vaccine may be possible, once a more comprehensive understanding of the process has been established’ (ah maybe these people are part of a giant experiment for vaccine developers?) End of quotes from this study.
*From a comment by 48 Malaba ‘Merck gets a tax deduction for giving ivermectin to Africa. While they do not get taxable cash from the sale of ivermectin, Merck does get a refund of $$ which would otherwise go to governments.Say an ivermectin pill costs 1 cent to make, and they give it away at 11 cents per pill. Merck then gets 10 cents in tax credits, which “after tax” , assum a 30% tax rate, in a simplified way equals a 3 cent profit per pill given to Africa for free.’ This for a drug that hundred of millions are advised to take every week! Merck is making a bomb.

From a study by the WHO declaring the success of IVM for mass community treatment; WHO treatment with IVM in affected populations looked at 9 worm and parasitic diseases. This was an observational study. It was not a randomised, placebo controlled experiment. The placebo effect accounts for up to 50% of any improvements seen in by both affecting the patient and the clinician. The diagnosis was made on microscopic examination of stool samples and clinical evaluation. These are both open to subjective interpretation and both microscopists and doctors knew that these people were being treated with IVM and the timing of the doses. The effects seen may also have been due to other changes, the continuing use of blanket spraying of insecticides, improvements in health care and sanitation. Some of the initial prevalence rates were already very low and at 9 months after 2 doses, the average the improvement in infection rate for the 9 conditions was 8.7%. Adverse reactions were seen in 9.4%.
The decreasing the prevalence of parasites by IVM may not be a good thing! Exposure to vaccines, toxins in the environment or from bites from insects who have bioaccumulated toxins may cause heavy metals to build up the body. Parasites may actually be helping the body to detox by acting as heavy metal and toxin filters. Parasites as heavy metal bioindicators in the shark Carcharhinus dussumieri from the Persian Gulf
IVM seems to be effective in treating individual cases of young worms and microfilariae in the skin, in a very small study with no blinding or placebo control. This is no evidence that it can prevent blindness. We do not now if the worms are causing blindness or are merely associated with it and are actually of benefit to the body in absorbing toxins. Treatment with IVM not only increases toxicity in the body in itself but also disrupts the microbiome and may rid the body of a potential toxin filtering mechanism afforded by ‘parasites’.

I'm wary when the WHO, UN and World Bank get involved in the developing world and tell us that such and such a thing has been eliminated, eradicated or prevented, and all thanks to them and their generosity. We know that the reduction in smallpox symptoms was due to better sanitation and child labour laws and had nothing whatsoever to do with the vaccine, however much pharma likes to crow that it did.

Antibiotics are effective at killing bacteria, though nobody would suggest mass, prophylactic treatment. The studies showing mass community reduction in prevalence (not necessarily better outcomes) are observational studies and are not placebo controlled (placebo effect accounts for up to 40% of the effect of a drug) and in any case only show a small reduction in already very rare diseases. Care must be taken with long term or frequent use of microbiome destroying antibiotics and anti-inflammatories. Long terms of non-steroidal anti-inflammatory drugs can destroy adrenal function for example.
How do we know that any reduction in ‘parasitic diseases’, are not due to other factors; such as less people living by rivers, changes in farming and employment practices, improvements in healthcare, sanitation and nutrition? Perhaps these diseases were caused by the imbalances in the ecosystems between flies, worms and humans due to Western colonisation, and the spraying with insecticides and other toxic chemicals in the first place.
Pharma has engineered a system where it is now seen as unethical to withdraw a treatment, though its efficacy has not been shown. In these papers we can clearly observe the key world players; initially identifying the tropical disease market, opening it up and then harvesting their monetary rewards, whilst claiming philanthropy.
IVM for ‘early treatment’ ie suppression of detox symptoms known as ‘covid 19’
A market and demand for Ivermectin (by banning its use) now seems to be deliberately being created as a prophylaxis for a disease that doesn’t even exist and to propagate the lie that the disease does exist. Some symptoms of detoxification such as inflammation may be suppressed by Ivermectin, but the symptoms are the healing. The body is trying to detox, just like using anti- diarrhoea or anti- vomiting drugs it means that the toxins will further build up in the body. If the body was going to ‘progress to disease’, it is because it needed to detox more. The body must be supported with nutrition and rest, not undermined with having its healing mechanisms suppressed.
IVM was not banned because it was effective but because for emergency use authorisations and the sole use of remdesivir as commanded by Fauci, there could not be another treatment available. If IVM had been tested against toxic and lethal remdesiver it would have appeared to be very effective whatever its actual value.

In this study on effectiveness of ivermectin in combination therapy for hypoxia , IVM is used with doxycyline, a broad spectrum antibiotic, zinc and vitamins D and C. It is known that though bacteria do not cause disease, they proliferate in diseased conditions, and antibiotics can appear to save lives for a short while, although the cause of the illness with still remain. If the benefit of IVM is anti-biotic its prophylactic used is certainly contraindicated. It is also impossible to separate any benefit of IVM from the vitamins. We know that the elderly in care homes especially are often malnourished and lack sunlight, especially when isolated during lockdowns, and benefit the most from vitamin supplementation.
In this study of 24 RCT's allegedly showing benefit of IVM it was claimed that IVM had a 62% relative improvement in death by any cause. These RCTs were comparing IVM with doxycycline vs HCQ with azithromycin, so the they don’t really tell us anything about IVM without antibiotics, or Ivermectin-azithromycin-cholecalciferol vs 7 controls in a small study or IVM with doxycycline with no deaths in either arms but improved 'viral clearance' by non specific PCR, or were using 'phone based' RCTs of IVM vs various treatments to show improvement in 'time to resolution' though the authors admit their study cannot recommend treatment with IVM. They are a mess of studies.
The certainty of most of the findings was low according to the authors of the meta-analysis due to severe limitations of the RCTs. They admit that ‘Overall interpretation of findings was hampered due to variability in the participants recruited, treatment regimen, and the care offered to those in control groups.’ The ‘care’ given to those in the non-IVM ‘control’ group was not known. It may have included combinations of drugs and toxic and lethal anti-’virals’. Even if IVM did reduce symptoms, this is not a good things. The detoxification and getting rid of dead cells is the healing, not the disease.
IVM as prophylaxis
The SAIVE Trial, Post-Exposure use of ivermectin in Covid-19 prevention: Efficacy and Safety Results this is a non-peer reviewed, pre print unverified report so I don’t know why I’m even talking about it, but for the sake of completeness. The results all rest on the PCR which we know does not show presence of a virus nor infection, and ‘viral loads’ ie equally meaningless number of PCR cycles. We do not know what the ‘placebo’ was nor what other interventions the controls were subject to. Taking IVM in this study appeared to reduce the chances of a non-specific PCR test. Assuming that the test picks up some sequences involved in the stress, detoxification and healing process, it would appear that IVM does indeed inhibit this process with an anti-inflammatory effect. Just like long term NSAIDS and antibiotics are very damaging, prophylactic use of IVM inhibiting the detoxification process to prevent a disease that doesn’t exist and retain toxins in the body seems to be a very bad idea.
Not properly looking into the research on something we just assume is good because the enemy says it’s bad is very foolish. We know that the narrative is clever enough to work out reverse psychology. Calling someone controlled opposition for saying anything negative about the holy grail of IVM is plain ridiculous.
IVM and male fertility
Ivermectin also appears to affect male fertility so would fit with the alleged depopulation plan Effect of ivermectin on male fertility and its interaction with P-glycoprotein inhibitor (verapamil) in rats and Effects of ivermectin and its combination with alpha lipoic acid on expression of IGFBP-3 and HSPA1 genes and male rat fertility; ‘The effects of administration of ivermectin (anthelmentic drug, Pgp substrate), either alone or simultaneously with verapamil (Pgp inhibitor) on male fertility were studied by determining mounting behavior, epididymal spermatozoal analysis, weight and histopathological examination of male reproductive organs and cytogenetic evaluation of meiotic chromosome’.’We concluded that ivermectin has slight effects on male fertility, but when taken with verapamil (used to prevent angina chest pain) induced adverse effects on meiosis and fertility.’ and ‘We concluded that ivermectin has undesirable effects on male fertility and altered expression of IGFBP-3 and HSPA1 genes in the testes, while the administration of alpha lipoic acid can ameliorate the adverse effects of ivermectin.’
Conclusion
Peter Daszak famously said that the plan was to get people addicted to a pan coronavirus vaccine and the money will flow in. Perhaps they’ll settle for getting the rest of us; all the ‘anti-vaxxers’ addicted to IVM. It seems to be working.
Jo
🐒
Wow!!. Very well written substack. I for one will not take!
Thanks Jo. I'll add this to my list of IVM resources.